Database Open Access
Simulated Obstructive Disease Respiratory Pressure and Flow
Jaimey Anne Clifton , Ella Frances Sophia Guy , Trudy Caljé-van der Klei , Jennifer Knopp , James Geoffrey Chase
Published: Nov. 13, 2023. Version: 1.0.0
When using this resource, please cite:
(show more options)
Clifton, J. A., Guy, E. F. S., Caljé-van der Klei, T., Knopp, J., & Chase, J. G. (2023). Simulated Obstructive Disease Respiratory Pressure and Flow (version 1.0.0). PhysioNet. https://doi.org/10.13026/xczc-3662.
Please include the standard citation for PhysioNet:
(show more options)
Goldberger, A., Amaral, L., Glass, L., Hausdorff, J., Ivanov, P. C., Mark, R., ... & Stanley, H. E. (2000). PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation [Online]. 101 (23), pp. e215–e220.
Abstract
The dataset presented is from 20 healthy adults at the University of Canterbury, where the tests were approved by its Human Research Ethics Committee (HREC) ethics. Data was collected using a modular device simulating the effects of Chronic Obstructive Pulmonary Disease (COPD) in healthy people, and in particular, the gas trapping due to airway collapse in expiration. Pressure and flow data were recorded in this trial using a y-split venturi with the device attached to the exhalatory outlet by the mouth. Data was collected using continuous positive airway pressure (CPAP) ventilation at positive end-expiratory pressure (PEEP) settings of 4 and 8 cmH20, and without the CPAP at zero end-expiratory pressure (ZEEP). The recording time for each test was 45 seconds with time in between each test to allow subjects to recover. Each subject filled out a de-identified demographic questionnaire to gather background information, including age, height, sex, and history of smoking, vaping, or asthma. The data collected is intended to be used as a preliminary validation method of respiratory computational models, where the device use avoids the need to test unhealthy people or use invasive methods.
Background
Respiratory diseases account for three of the top ten causes of death worldwide [1]. There are two different classifications of respiratory disease, obstructive and restrictive lung disease. Obstructive lung disease creates an expiratory flow limitation due to an obstruction and restrictive lung disease results in a reduced inspiratory capacity [2]. Diseases can be either be classified as restrictive, obstructive, or a combination of both.
COPD in particular is predominantly a non-reversible obstructive disease and is the third leading cause of death worldwide [1]. It is a growing healthcare concern, with increasing rates of smoking, pollution, and obesity, adding to the rising numbers of this disease [3-5]. In 2012, COPD accounted for 6% of deaths worldwide [4]. COPD is treatable and preventable, so this percentage could be decreased with early detection and diagnostic methods, as early-stage COPD goes largely undiagnosed [4, 6-8].
The diagnosis of COPD is carried out in clinical settings using spirometry, other lung function tests, and sometimes imaging, such as x-ray or CT scans [7]. When diagnosing COPD, key factors clinicians consider include the patient’s medical history and any history of smoking or exposure to environmental factors [9]. Spirometry is a readily available lung function test using a combination of forced breathing manoeuvres to measure changes in lung volumes [10]. Spirometry specifically measures the forced vital capacity of the lungs (FVC) and the forced expiratory volume of the lungs in one second (FEV1). FEV1 and FVC are measured after a maximal inspiration and forced expiration [7, 10, 11]. FEV1 is the volume of air expired in the first second and FVC is the total exhaled volume of air during exhalation [10]. COPD presents as a decreased FVC and FEV1, and thus the forced expiratory ratio (FER) FEV1/FVC is also used in the diagnosis [12].
To determine if the airway obstruction is reversible or non-reversible these tests are conducted before and after bronchodilators or corticosteroids have been administered. If the FEV1 remain less than 80% and the FER ratio less than 0.7 after conducting these tests with bronchodilators it is indicative of a non-reversible airflow obstruction [4, 6, 9, 10]. Spirometry in the diagnosis of COPD has good sensitivity, but poor specificity, as in some cases it can be hard to differentiate between COPD and asthma [4, 9, 11]. Therefore, it is usually used in conjunction with another lung function test, such as body plethysmography [4].
Overall, lung function tests such as spirometry are useful diagnostic tools. However, due to the low specificity and the inability to be used by young children, elderly, and those with severe illness who cannot fully perform some of the required breathing maneuvers, it can require further tests, all of which add expense and time. Computational respiratory models offer the opportunity to predict patient-specific respiratory metrics directly associated with COPD lung mechanics and disease progression, and to do so via normal breathing maneuvers, reducing time and cost [13, 14].
The data presented is to be used in the initial preliminary validation of respiratory models to avoid the unnecessary burden of testing on unhealthy people with COPD. Currently, testing respiratory models requires using data collected from unhealthy people using potentially invasive methods. Using devices to simulate the disease state, or its key components, as in this data, enables healthy people to produce data very similar to those with COPD, mitigating experimental risk and effort.
Methods
The data was collected using venturi flow sensors taken from an existing design and a device designed to simulate COPD [15, 16]. The simulation device was a modular device attached to the exhalation side of the y-split tube of the flow sensors to allow inhalation to remain unchanged. A filter was attached to the patient side of the flow sensor, to collect data the test subject used a mouthpiece attached to the filter and a nose clip to ensure minimal air was lost. The mouthpiece was used instead of CPAP mask as the simulation device required a larger amount of force to be used on exhalation which would result in mask air leakage.
The modular device consisted of two main components, a fixed high resistance outlet and an elastic free volume [16]. During exhalation the air initially entered the low resistance elastic free volume, as the pressure in the chamber increased the air was diverted out the fixed high resistance outlet. This initial free volume followed by a high resistance outlet creates the nonlinearity of an obstructed airway and expiratory gas trapping seen in COPD, and thus a nonlinear pressure-flow (or P-Q) expiratory curve [17].
The trial protocol consisted of four different tests. The first was to breathe through the flow sensors for 45sec without the simulator device attached to get a control baseline. This baseline tests was completed at ZEEP (zero end-expiratory pressure) and two positive pressure PEEP (positive end-expiratory pressure) levels of 4cmH20, and 8cmH20 generated by a CPAP machine (SleepStyle SPSCAA, Fisher and Paykel Healthcare, East Tamaki, Auckland, NZ). After this baseline set of tests, the modular simulation device was attached using the smallest free volume size of 200ml. The same three PEEP level tests (0, 4, 8 cmH2O) were conducted. The series was repeated again for the 250ml and the 300ml elastic free volume sizes. Each test subject was given time in between trial to catch their breath and take a break for as long as required.
Data Description
The data collected is from 20 healthy subjects, 10 females and 10 males, with no self-identified serious underlying health condition. This study was conducted at the University of Canterbury low risk clinical unit with ethics granted by the human research ethics committee (HREC). The subjects were given written information and a consent form then were given a de-identified number and asked to fill out a demographic questionnaire asking for demographic information including age, height, sex, any history of smoking or asthma. This data is provided in an excel spreadsheet labelled ‘COPD_Demographic.xlsx’. Columns A:J of this file contain the following information: Subject Number, age [years], gender, height [cm], history of smoking, frequency of smoking, history of vaping, frequency of vaping, any underlying or known heart condition, history or diagnosis of asthma. Any subject with a known underlying heart condition or severe asthma was excluded from this trial.
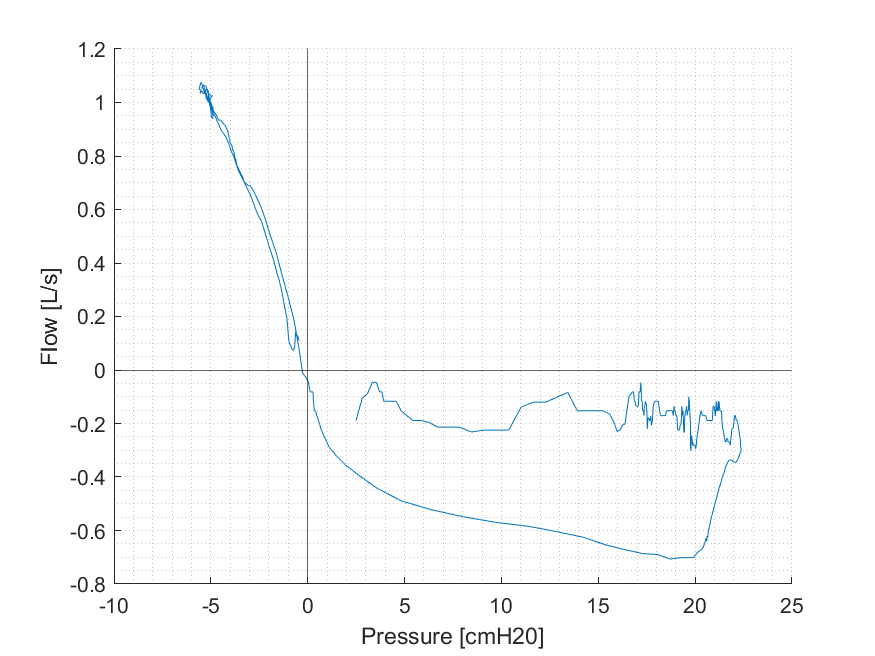
The processed data is saved as .csv files in the folder labelled ‘PQ_ProcessedData’. Files are labelled with the subject number (1 through to 20), PEEP used (0cmH2O, 4cmH2O, or 8cmH2O) and simulation device size (0ml, 200ml, 250ml, or 300ml) for example 'ProcessedCOPD_Subject20_8cmH2O_300ml.csv'. The csv files contain time [s], pressure [cmH2O], flow [L/s], tidal volume [L], inspiratory indices, and weight [kg]. The raw data is saved under the folder ‘PQ_rawData’ as csv files. The files are saved under the same method of subject number (1 through to 20), PEEP used (0cmH2O, 4cmH2O, or 8cmH2O) and simulation device size (0ml, 200ml, 250ml, or 300ml) for example 'COPDTrial2023_Subject1_0cmH2O_0mL.csv'. The files contain time [s], raw gauge pressure [cmH2O], the inspiratory differential pressure [cmH2O], and expiratory differential pressure [cmH2O]. These files are saved with the relevant units 'COPDTrial2023_Subject1_0cmH2O_0mL.csv' and as the raw ADC outputs 'COPDTrial2023_Subject1_0cmH2O_0mL_raw.csv'. The MATLAB code ‘PQ_Loop.m’ is an example section of MATLAB code used to plot ‘figure_1’ the first breath from subject 1, 0cmH20 PEEP, and 300ml device as a PQ loop showing the expected resulting non-linear resistance and obstructed airway lobe on expiration.
The first intended use of this dataset is the initial validation and development of respiratory models, before testing the model using data collected from people who have COPD. Second, and more generalisable, this device allows non-invasive, patient specific, repeatable data to be created for COPD or used to test new devices or therapies without testing on vulnerable patients with COPD. Critically, it is data with an exact match healthy individual comparator, which is the same subject without the device. This data set has both, where the control baseline data is without the device, and is thus an initial data set with its unique comparator and useful in its own right. Finally, although this is a small dataset size it allows initial biomarkers to be identified using respiratory models. All hardware is available opensource, modifiable, and the trial is easily repeatable meaning this data can be added to in the future.
Usage Notes
The intended use of this dataset is the initial validation and validation of respiratory mechanics models, specifically modelling changes in pulmonary physiology in obstructive disease (e.g. COPD). The dataset is from a pilot study which collects data from healthy people with a device that simulates the pressure and flow profiles of COPD [16]. Ethics for the trial were accepted by the University of Canterbury Human Ethics Committee (HREC) (ref: HREC 2022/26/LR) with amendments accepted on the 17th February 2023. Development of COPD respiratory models commonly involves initially using a mechanical lung. However, this does not account for subject variability and does not allow patient specific data to be collected. This dataset provides an additional patient specific, variable resource to aid in the model development.
Additional reuse potential of this dataset could be comparison to different disease states of COPD as the hardware uses three different free volume sizes (which is also modifiable to incorporate more sizes). The dataset could be used in comparison to existing COPD data to identify similarities and differences in disease biomarkers or states. The hardware used in the trail is also all published open-source access therefore this dataset can be added to, with the same free volume sizes and resistances used or with modifications made.
The data is easily replicable as it has been collected using open-source devices and was tested on healthy people and non-invasive methods [15, 16]. 3D print files and instructions are available for the simulation device and data collection device [15, 16]. Thus, allowing the device to easily be modified for different applications and disease states. The resultant P-Q breath curves generated from the collected dataset, show a nonlinear resistance lobe on exhalation that mimic the nonlinearity in resistance created by gas trapping and an obstructed airway seen in COPD [14, 17]. Thus, validating the efficacy and utility of the device.
Ethics
Ethical consent was granted for the trial by the Human Ethics Committee at the University of Canterbury (Ref: HREC 2022/26/LR), with amendments accepted on the 17th February 2023.
Acknowledgements
This work was funded by a University of Canterbury Doctoral Scholarship and the EU H2020 R&I programme (MSCA-RISE-2019 call) under grant agreement #872488 — DCPM.
Conflicts of Interest
The authors have no conflicts of interest to declare.
References
- S. M. Levine and D. D. Marciniuk, "Global Impact of Respiratory Disease: What Can We Do, Together, to Make a Difference?," Chest, vol. 161, no. 5, pp. 1153-1154, 2022/05/01/ 2022, doi: https://doi.org/10.1016/j.chest.2022.01.014. [Accessed 27/10/23]
- J. H. T. Bates, Lung mechanics: an inverse modeling approach. Cambridge University Press, 2009.
- T. L. Petty, "The history of COPD," International Journal of Chronic Obstructive Pulmonary Disease, vol. 1, no. 1, pp. 3-14, 2006/01/01 2006, doi: https://doi.org/10.2147/copd.2006.1.1.3. [Accessed 27/10/23]
- P. Venkatesan, "GOLD COPD report: 2023 update," The Lancet Respiratory Medicine, vol. 11, no. 1, p. 18, 2023/01/01/ 2023, doi: https://doi.org/10.1016/S2213-2600(22)00494-5. [Accessed 27/10/23]
- M. Aghapour et al., "Role of air pollutants in airway epithelial barrier dysfunction in asthma and COPD," European Respiratory Review, vol. 31, no. 163, p. 210112, 2022, doi: https://doi.org/10.1183/16000617.0112-2021. [Accessed 27/10/23]
- C.-H. Lin, S.-L. Cheng, C.-Z. Chen, C.-H. Chen, S.-H. Lin, and H.-C. Wang, "Current Progress of COPD Early Detection: Key Points and Novel Strategies," International Journal of Chronic Obstructive Pulmonary Disease, vol. 18, pp. 1511-1524, 2023/12/31 2023, doi: https://doi.org/10.2147/COPD.S413969. [Accessed 27/10/23]
- N. G. Csikesz and E. J. Gartman, "New developments in the assessment of COPD: early diagnosis is key," International Journal of Chronic Obstructive Pulmonary Disease, vol. 9, pp. 277-286, 2014/12/06 2014, doi: https://doi.org/10.2147/COPD.S46198. [Accessed 27/10/23]
- S. Rennard et al., "Introducing the COPD Foundation Guide for Diagnosis and Management of COPD, Recommendations of the COPD Foundation," COPD: Journal of Chronic Obstructive Pulmonary Disease, vol. 10, no. 3, pp. 378-389, 2013/06/01 2013, doi: https://doi.org/10.3109/15412555.2013.801309. [Accessed 27/10/23]
- C. E. Bolton, A. A. Ionescu, P. H. Edwards, T. A. Faulkner, S. M. Edwards, and D. J. Shale, "Attaining a correct diagnosis of COPD in general practice," Respiratory Medicine, vol. 99, no. 4, pp. 493-500, 2005/04/01/ 2005, doi: https://doi.org/10.1016/j.rmed.2004.09.015. [Accessed 27/10/23]
- T. J. Barreiro and I. Perillo, "An approach to interpreting spirometry," (in eng), Am Fam Physician, vol. 69, no. 5, pp. 1107-14, Mar 1 2004. [Online]. Available: https://www.aafp.org/pubs/afp/issues/2004/0301/p1107.html. [Accessed 27/10/23]
- E. Andreeva, M. Pokhaznikova, A. Lebedev, I. Moiseeva, O. Kuznetsova, and J.-M. Degryse, "Spirometry is not enough to diagnose COPD in epidemiological studies: a follow-up study," npj Primary Care Respiratory Medicine, vol. 27, no. 1, p. 62, 2017/11/14 2017, doi: https://doi.org/10.1038/s41533-017-0062-6. [Accessed 27/10/23]
- D. P. Johns, J. A. Walters, and E. H. Walters, "Diagnosis and early detection of COPD using spirometry," (in eng), J Thorac Dis, vol. 6, no. 11, pp. 1557-69, Nov 2014, doi: https://doi.org/10.3978/j.issn.2072-1439.2014.08.18. [Accessed 27/10/23]
- E. F. S. Guy, J. G. Chase, J. L. Knopp, and G. M. Shaw, "Quantifying ventilator unloading in CPAP ventilation," Computers in Biology and Medicine, vol. 142, p. 105225, 2022/03/01/ 2022, doi: https://doi.org/10.1016/j.compbiomed.2022.105225. [Accessed 27/10/23]
- T. Lerios, J. L. Knopp, L. Holder-Pearson, E. F. S. Guy, and J. G. Chase, "An identifiable model of lung mechanics to diagnose and monitor COPD," (in eng), Comput Biol Med, vol. 152, p. 106430, Jan 2023, doi: https://doi.org/10.1016/j.compbiomed.2022.106430. [Accessed 27/10/23]
- E. F. S. Guy, J. A. Clifton, J. L. Knopp, L. R. Holder-Pearson, and J. G. Chase1, "Respiratory pressure and split flow data collection device with rapid occlusion attachment," HardwareX, vol. In Review, 2023.
- J. A. Clifton, E. F. S. Guy, J. L. Knopp, and J. G. Chase, "Obstructive Respiratory Disease Simulation Device," HardwareX, vol. In Review, 2023.
- J. A. Clifton et al., "Physical Simulation of Obstructive Respiratory Disease " IFAC-PapersOnLine, vol. In Review, 2023.
Access
Access Policy:
Anyone can access the files, as long as they conform to the terms of the specified license.
License (for files):
Creative Commons Attribution 4.0 International Public License
Discovery
DOI (version 1.0.0):
https://doi.org/10.13026/xczc-3662
DOI (latest version):
https://doi.org/10.13026/v59r-fy88
Corresponding Author
Files
Total uncompressed size: 153.0 MB.
Access the files
- Download the ZIP file (34.2 MB)
-
Download the files using your terminal:
wget -r -N -c -np https://physionet.org/files/simulated-obstructive-disease/1.0.0/
| Name | Size | Modified |
|---|---|---|
| PQ_ProcessedData | ||
| PQ_RawData | ||
| COPD_Demographic.csv (download) | 1.1 KB | 2023-10-19 |
| LICENSE.txt (download) | 14.5 KB | 2023-11-11 |
| PQ_Loop.m (download) | 922 B | 2023-10-26 |
| README.txt (download) | 1.5 KB | 2023-10-26 |
| SHA256SUMS.txt (download) | 84.4 KB | 2023-11-13 |
| figure_1.png (download) | 37.1 KB | 2023-10-26 |
{kind=link}
{kind=link}