Database Open Access
Respiratory and heart rate monitoring dataset from aeration study
Ella Frances Sophia Guy , Isaac Flett , Jaimey Anne Clifton , Trudy Caljé-van der Klei , Rongqing Chen , Jennifer Knopp , Knut Moeller , James Geoffrey Chase
Published: March 20, 2024. Version: 1.0.0
When using this resource, please cite:
(show more options)
Guy, E. F. S., Flett, I., Clifton, J. A., Caljé-van der Klei, T., Chen, R., Knopp, J., Moeller, K., & Chase, J. G. (2024). Respiratory and heart rate monitoring dataset from aeration study (version 1.0.0). PhysioNet. https://doi.org/10.13026/e4dt-f689.
Please include the standard citation for PhysioNet:
(show more options)
Goldberger, A., Amaral, L., Glass, L., Hausdorff, J., Ivanov, P. C., Mark, R., ... & Stanley, H. E. (2000). PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation [Online]. 101 (23), pp. e215–e220.
Abstract
A study was conducted to collect respiratory pressure and flow data for model-based assessment, alongside electrical impedance tomography (EIT) aeration, electrocardiogram (ECG), and heart-rate belt (HRB) data. A 20 subjects set was selected with no known significant respiratory abnormalities, under University of Canterbury Human Research Ethics Committee (HREC) consent (HREC 2023/30/LR-PS). Subject demographic data was collected using a combination of measurements and a self-reported questionnaire. Subject demographic information to ascertain: sex; height; weight; age; any history of asthma, smoking, or vaping; and approximate thoracic cage and breast tissue volumes. The trial was setup with subjects breathing through the pressure and flowmeter using a full-face mask and filter. Inspiratory and expiratory flow were separated using one-way valves for measurement purposes and both ports were rapidly occluded every 200ms to generate passive mechanics assessment intervals. A continuous positive airway pressure (CPAP) machine was used to provide positive airway pressure (PEEP) in series with the inspiratory port. Three trials were conducted per subject. Two of which, involved increasing PEEP (0, 4, and 8 cmH2O), and in one of which subjects were asked to perform two 10s breath holds at each level. The third was a recording of three forced expiratory manoeuvres (FEM). These tests were conducted to provide an initial comparison of current respiratory techniques to model-based methods, which aims to inform the design of future clinical testing on subjects with known respiratory abnormalities.
Background
Respiratory physiological model-based analyses methods have undergone significant development since the invention of common respiratory testing and treatment tools [1-12]. However, the use of these models in clinical practice is limited [13]. The outlined dataset was conducted as a proof-of concept test of prototype monitoring methods, in conjunction with an approximation of current methods, within a healthy population [14, 15]. The analyses of which, hopes to inform the design of clinical testing for implementation of model-based assessment to care practice.
Respiratory system dysfunction can be physiologically categorised by obstructive, restrictive, or neuromuscular abnormalities [16-18]. However, many respiratory diseases can cause multiple abnormalities across multiple categories [19, 20]. Additionally, in a clinical context, a respiratory disease also rarely occurs in isolation, and the elucidation of symptoms from associated cardiovascular and/or additional respiratory diseases is difficult without direct measurement tools [19-23]. However, direct measurement of respiratory function, through methods such as an oesophageal balloon are highly invasive and can themselves cause respiratory abnormalities [24, 25]. Thus, direct measurement is impractical in most cases of spontaneous breathing (un-intubated) patients.
Therefore, the application of model-based methods in a clinical context has the potential to improve the quality and frequency of data provided to clinicians and patients. Hence, increase the ability for both clinicians and patients to make informed care decisions. Thus, the outlined dataset was collected to justify and inform clinical testing of model-based monitoring methods.
Methods
Pressure and flow data for model-based analysis was collected through a custom calibrated venturi-based flow and pressure sensor device [14], with an added inspiratory flow pathway shutter. The device split inspiration and expiration pathways using one-way valves and rapidly occluded the expiratory pathway [14]. A filter (R » 0.5 cmH2Os/L) and full-face mask (with sealed expiratory venting ports) were connected in series at the patient interface. A CPAP machine (SleepStyle SPSCAA, Fisher and Paykel Healthcare, East Tamaki, Auckland, NZ) provided the set PEEPs through an adapter connected to the inspiratory pathway shutter.
An electrical impedance tomography (EIT) device (Dräger PulmoVista 500, Dräger, Lübeck, Germany) was used to collect aeration data through the trials. The subject was seated during testing and the EIT electrode belt was placed around the chest at axilla level in the same plane as the chest width and depth data. The EIT reference electrode was placed on the subject’s abdomen in line with the umbilicus and on the parasagittal plane. The EIT belt was calibrated immediately prior to the first trial (PEEP) and recordings were then taken separately for each trial, in the same manner as pressure and flow data collection.
Heart-rate monitoring (HRM) data was recorded from custom ECG [26-28], custom PPG [29, 30], and heart-rate belt (Garmin HRM Dual, Garmin Ltd, Olathe, KS, USA) systems. ECG electrodes were placed under both left and right clavicles in the space between the shoulder joint and thoracic cage, with the third electrode located on the abdomen in line with the umbilicus and on the parasagittal plane, on the opposite side to the EIT reference electrode. The PPG sensor device was attached to the subjects left index finger. The heart-rate belt was placed around the subject’s chest under the pectoral muscles. Recordings were taken continuously over all three trials. In some cases, ECG and PPG recordings were paused between trials, which is reflected in the time arrays.
Pressure and flow data was collected using a MATLAB (Matlab 2021b, The Mathworks Inc, Natick, MA, USA) script ('DataCollection_PQ.m’), the Dräger PulmoVista 500, GUI for ECG and PPG data collection written in Python (Python 3.9, The Python Software Foundation, Wilmington, DE, US), and the Garmin heart-rate belt. In the first trial (‘PEEP’) data was recorded from subjects breathing normally at rest without CPAP (at ZEEP) for 1 min, then at PEEP settings of 4 and 8 cmH2O for 1 min each, before a final 1 min recording without CPAP. Between each level, researcher setting adjustment intervals (of 30 s each) were included in which continuous data collection continued. In the second trial (‘PEEP_BH’), the first trial protocol was repeated, with the addition of the subject being asked to include two breath holds of approximately 10 seconds at each level. The subject was provided with a stopwatch to time these breath holds. The final trial (‘FEM’), consisted of a 60 second recording in which the subject was asked to perform three forced expiratory manoeuvres in their own time. These were coached to subjects as breathing out as much as possible to empty their lungs and then to take the biggest breath they possibly could. Subjects were allowed a self-determined recovery window between trials.
Data Description
Respiratory and cardiovascular data were collected from 20 subjects, split evenly by sex. Demographic data for the 20 subjects was self-reported and measured and is included as a spreadsheet ('subject-info.csv') by subject number. Sex [M/F], height[cm], weight [kg], age [years], bra size (if applicable), and data on history of asthma, smoking, and vaping was self-reported using a questionnaire, with height and weight measurement devices made available. Chest width (back size) and depth (sternum to spine size) values were measured by the two researchers conducting testing. Approximations of chest and breast size from width and depth were taken to assess the influence of added tissue and thoracic cage shape on EIT accuracy, which currently assumes thoracic cross-sectional boundaries.
The raw data collected is saved in three folders: the pressure, flow, and dynamic circumference data is saved in 'PQ_rawData'; the EIT aeration data is saved in 'EIT_rawData'; and the heart-rate data is saved in ‘HRM_rawData’. The 'PQ_rawData' folder contains both raw data (e.g. ‘Subject1_PEEP_raw.csv’) and data processed into relevant units (e.g. ‘Subject1_PEEP.csv’). Files are saved by subject number (‘1’ through to ‘20’) and trial type (‘PEEP’, ‘PEEP_BH’, and ‘FEM’). Files contain the following data sampled at 100Hz: time, gauge pressure, inspiratory differential pressure, expiratory differential pressure and recording start time ('HH:mm:ss' format). Code to collect this data in MATLAB ('DataCollection_PQ.m’) is included in the 'Code' folder. The 'EIT_rawData' folder contains the EIT device data (e.g. ‘S01_PEEP.bin'), saved by subject number (‘01’ through to ‘20’) and trial type (‘PEEP’, ‘PEEP_BH’, and ‘FEM’). These files contain data as a matrix of pixel values representing regional aeration for a cross-sectional image (32x32 frame) over time (with 50Hz sampling). A function to read these files in MATLAB is included in the 'Code' folder as ‘read_binData.m’. The 'HRM_rawData' folder contains subfolders: ‘ECG’; ‘PPG’; and ‘HRB’. Each of these folders contains 1 file per subject which includes data from all their respective trials. The 'ECG' folder contains electrocardiography data by subject number (‘S01_ECG.csv’) which consists of time array data in 'HH:mm:ss.SSS' format and a corresponding ECG data array [mV]. The 'PPG' folder contains photoplethysmography data by subject number (‘S01_PPG.csv’) which time array data in 'HH:mm:ss.SSS' format and three corresponding PPG data arrays for each of the three LED sensors on the device ('PPG0','PPG1', and 'PPG2'). ECG and PPG data was collected using using a GUI written in Python 3.9 code[26-30]. The 'HRB' folder contains heart rate belt data by subject number (e.g. '3.txt'). These files contain a data time array in 'HH:mm:ss.SSSSSS''Z' format, a message ID array, a RR interval data array, and a heart-rate data array [BPM]. Heart-rate belt data was not collected for subjects 1 and 2.
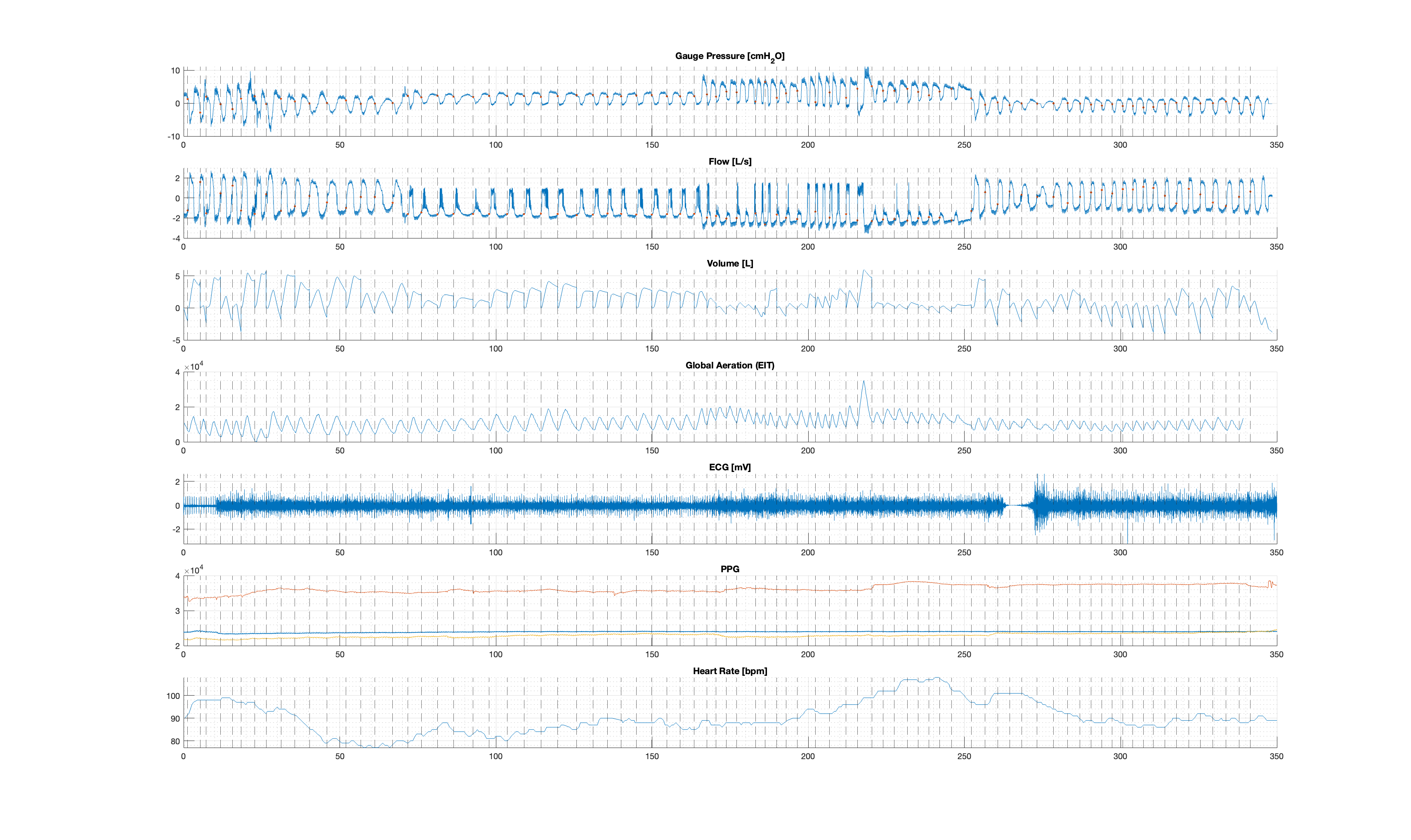
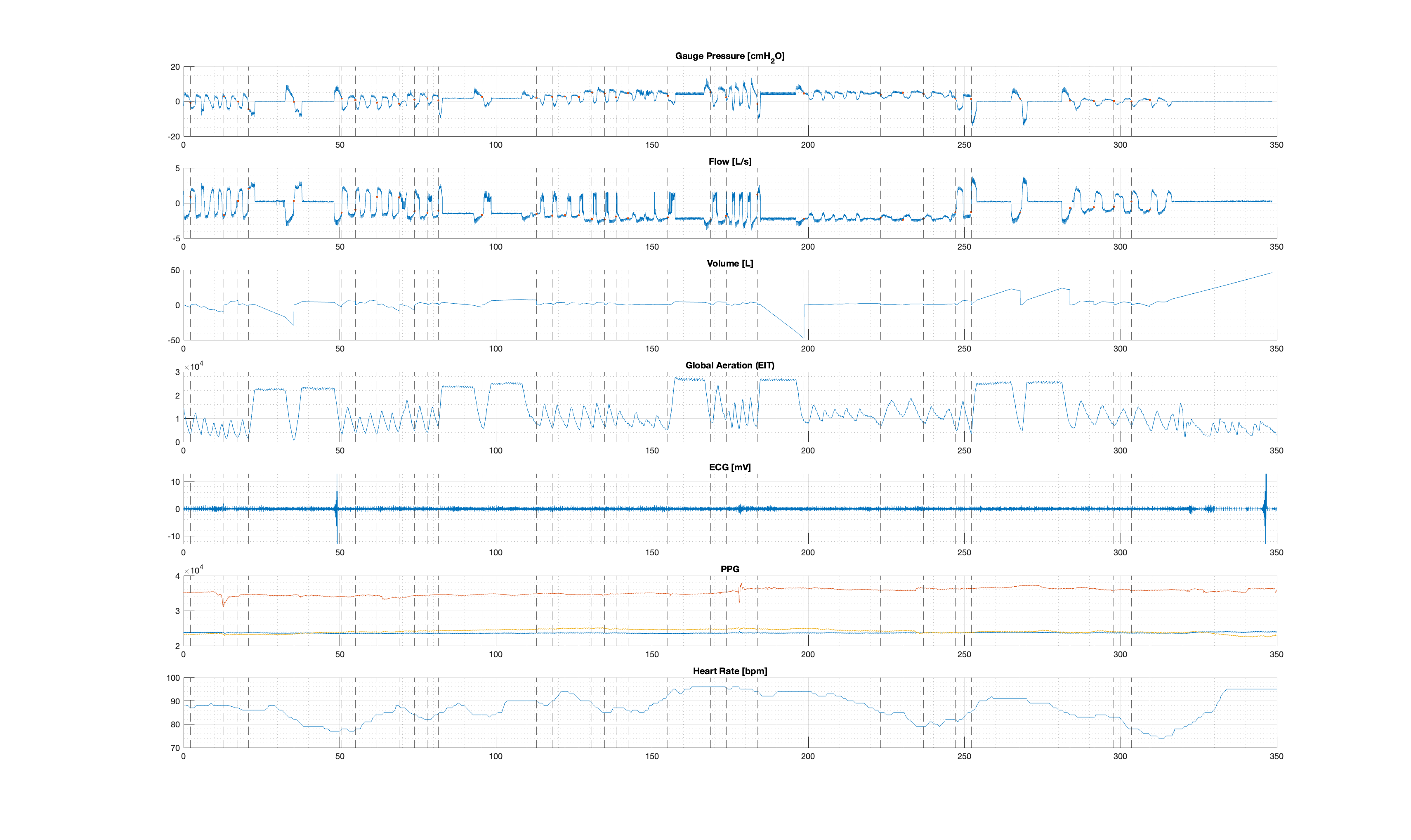
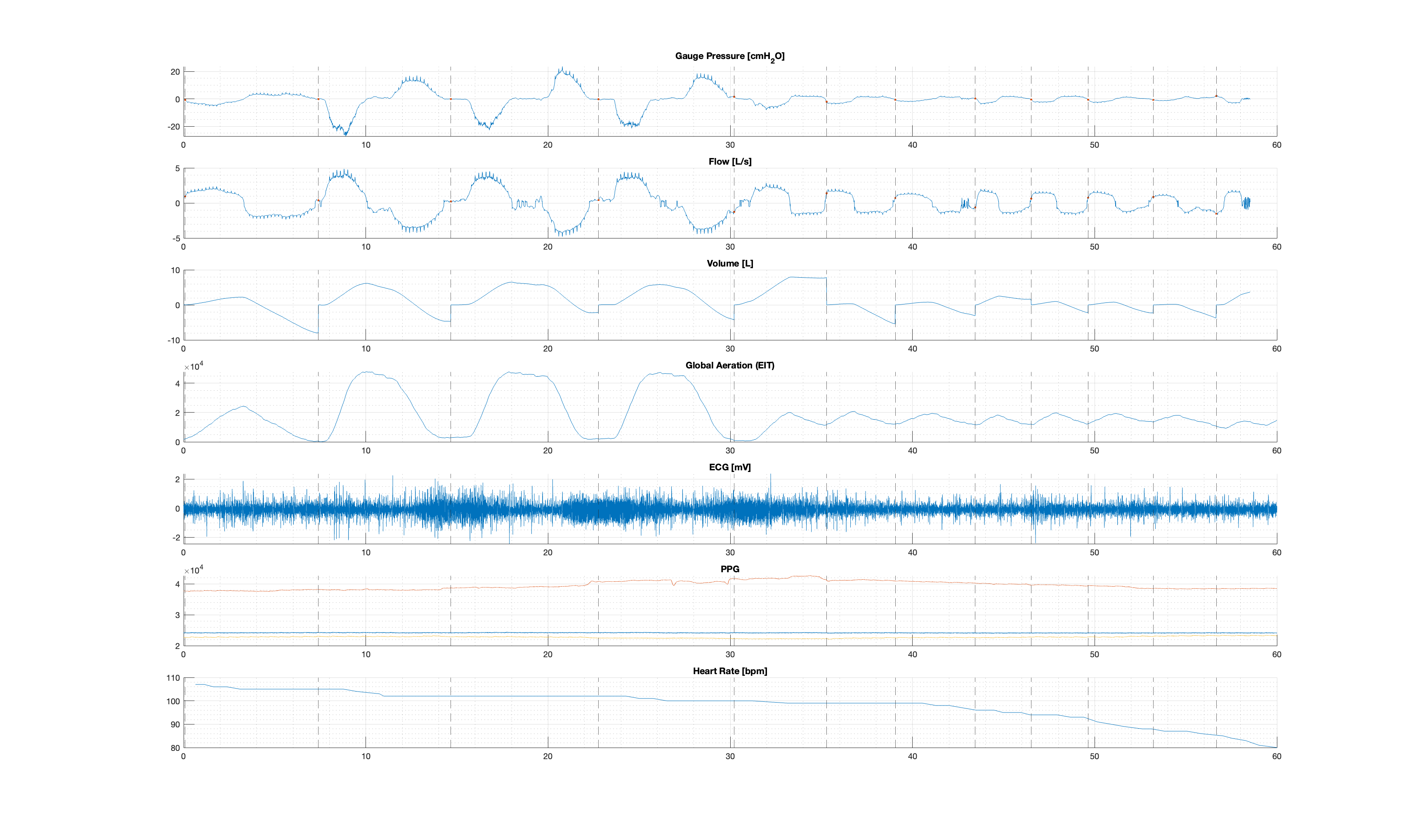
The combined and processed data is saved in the 'Processed_Dataset' folder by subject number and trial type (e.g. ‘ProcessedData_Subject01_PEEP.csv’). Processed data files contain: Pressure, flow, and tidal volume data time [s]; gauge pressure [cmH2O]; inspiratory differential pressure [cmH2O]; expiratory differential pressure [cmH2O]; flow [L/s]; tidal volume [L]; pressure, flow, and tidal volume data inspiratory indices; aeration data time [s]; global aeration; ECG data time [s]; ECG signal [mV]; PPG data time [s]; the three PPG signals (PPG0, PPG1, and PPG2); heart rate belt data time [s]; heart rate belt heartrate [bpm]; heart rate belt RR Interval [ms]. With the exception of Subjects 1 and 2 who have the above data, with the exception of heartrate belt data. Data processing code ('DataProcessing.m') is included in the ‘Code’ folder. Example figures of the processed dataset for Subject 3 for each trial are also included ('Figure1.png', 'Figure2.png', and 'Figure3.png'), alongside figure generation code ('FigureGeneration.m').
Usage Notes
This dataset was collected to be used to justify and inform the development of clinical testing. As well as to validate, optimise, and improve model-based methods for use in a clinical setting. The trial 20 subjects, evenly split by sex, as a proof-of-concept cohort to minimise the burden on disease populations. The inclusion of basic cardiac monitoring was also included for preliminary analysis on the impact of cardiac function on respiratory analyses, in order to identify any required inputs for both pressure and flow model-based or EIT respiratory analyses methods.
The University of Canterbury Human Research Ethics Committee (HREC) granted ethical consent for this trial (HREC 2023/30/LR-PS). This trial builds from a base of trials conducted to establish and validate model-based respiratory assessment methods for clinical implantation [31-36], conducted under similar ethical consent (HREC 2023/04/LR-PS and HREC 2020/14/LR). Pressure and flow measurement hardware and software is available open-access [37],with design files and instructions available [14]. Details of the ECG hardware and software are published [26-30]. and results could be similarly reproduced using commercially available models. Additionally, descriptions and information on reproducing PPG data collection hardware is published [29, 30]. Hence, results can be readily reproduced, augmented, and modified in future research applications. This dataset also contains data collection, processing, and visualisation MATLAB code.
Ethics
Ethical consent for the trial was granted by the Human Research Ethics Committee at the University of Canterbury (Ref: HREC 2023/30/LR-PS) on 24 April 2023.
Acknowledgements
This work was funded by a University of Canterbury Doctoral Scholarship and the EU H2020 R&I programme (MSCA-RISE-2019 call) under grant agreement #872488 — DCPM.
Conflicts of Interest
The authors have no conflcits of interest to declare.
References
- J. L. Knopp, J. G. Chase, K. T. Kim, and G. M. Shaw, "Model-based estimation of negative inspiratory driving pressure in patients receiving invasive NAVA mechanical ventilation," Computer Methods and Programs in Biomedicine, vol. 208, p. 106300, 2021.
- S. E. Morton et al., "Optimising mechanical ventilation through model-based methods and automation," Annual Reviews in Control, vol. 48, pp. 369-382, 2019.
- S. L. Howe et al., "Measuring lung mechanics of expiratory tidal breathing with non-invasive breath occlusion," BioMedical Engineering OnLine, vol. 19, no. 1, p. 32, 2020.
- J. H. Bates, Lung mechanics: an inverse modeling approach. Cambridge University Press, 2009.
- J. G. Chase et al., "Next-generation, personalised, model-based critical care medicine: a state-of-the art review of in silico virtual patient models, methods, and cohorts, and how to validation them," Biomedical engineering online, vol. 17, no. 1, pp. 1-29, 2018.
- Y. S. Chiew, J. G. Chase, G. M. Shaw, A. Sundaresan, and T. Desaive, "Model-based PEEP optimisation in mechanical ventilation," Biomedical engineering online, vol. 10, pp. 1-16, 2011.
- Y. S. Chiew et al., "Time-varying respiratory system elastance: a physiological model for patients who are spontaneously breathing," PloS one, vol. 10, no. 1, p. e0114847, 2015.
- S. E. Rees et al., "Using physiological models and decision theory for selecting appropriate ventilator settings," Journal of clinical monitoring and computing, vol. 20, pp. 421-429, 2006.
- S. E. Rees, "The Intelligent Ventilator (INVENT) project: The role of mathematical models in translating physiological knowledge into clinical practice," Computer methods and programs in biomedicine, vol. 104, pp. S1-S29, 2011.
- T. Lerios, J. L. Knopp, L. Holder-Pearson, E. F. Guy, and J. G. Chase, "An identifiable model of lung mechanics to diagnose and monitor COPD," Computers in Biology and Medicine, vol. 152, p. 106430, 2023.
- B. Suki and J. Bates, "A nonlinear viscoelastic model of lung tissue mechanics," Journal of Applied Physiology, vol. 71, no. 3, pp. 826-833, 1991.
- S. E. Morton et al., "Prediction of lung mechanics throughout recruitment maneuvers in pressure-controlled ventilation," Computer Methods and Programs in Biomedicine, vol. 197, p. 105696, 2020.
- Y. S. Chiew et al., "Clinical application of respiratory elastance (CARE trial) for mechanically ventilated respiratory failure patients: A model-based study," IFAC-PapersOnLine, vol. 51, no. 27, pp. 209-214, 2018.
- E. F. Guy, J. A. Clifton, J. L. Knopp, L. R. Holder-Pearson, and J. G. Chase, "Respiratory pressure and split flow data collection device with rapid occlusion attachment," HardwareX, p. e00489, 2023.
- E. F. S. Guy, J. L. Knopp, T. Lerios, and J. G. Chase, "Model-based Identification of Work of Breathing in CPAP Ventilation of Healthy Adults " IFAC-PapersOnLine 2023, doi: https://doi.org/10.1016/j.ifacol.2023.10.1107.
- T. Des Jardins and G. G. Burton, Clinical Manifestations & Assessment of Respiratory Disease-E-Book. Elsevier Health Sciences, 2023.
- R. Pellegrino et al., "Interpretative strategies for lung function tests," European respiratory journal, vol. 26, no. 5, pp. 948-968, 2005.
- S. C. Bourke, "Respiratory involvement in neuromuscular disease," Clinical Medicine, vol. 14, no. 1, p. 72, 2014.
- M. Boentert, S. Wenninger, and V. A. Sansone, "Respiratory involvement in neuromuscular disorders," Current opinion in neurology, vol. 30, no. 5, pp. 529-537, 2017.
- Z. S. Gardner, G. L. Ruppel, and D. A. Kaminsky, "Grading the severity of obstruction in mixed obstructive-restrictive lung disease," Chest, vol. 140, no. 3, pp. 598-603, 2011.
- E. Diaz-Guzman, K. McCarthy, A. Siu, and J. K. Stoller, "Frequency and causes of combined obstruction and restriction identified in pulmonary function tests in adults," Respiratory care, vol. 55, no. 3, pp. 310-316, 2010.
- F. H. Rutten, M. J. M. Cramer, J. W. J. Lammers, D. E. Grobbee, and A. W. Hoes, "Heart failure and chronic obstructive pulmonary disease: an ignored combination?," European journal of heart failure, vol. 8, no. 7, pp. 706-711, 2006.
- F. E. Campbell, "Cardiac effects of pulmonary disease," Veterinary Clinics of North America: Small Animal Practice, vol. 37, no. 5, pp. 949-962, 2007.
- J. L. Knopp, E. Guy, K. T. Kim, G. M. Shaw, and J. G. Chase, "B-spline modelling of inspiratory drive in NAVA-ventilated patients," IFAC-PapersOnLine, vol. 54, no. 15, pp. 103-108, 2021.
- X.-M. Sun et al., "Use of esophageal balloon pressure-volume curve analysis to determine esophageal wall elastance and calibrate raw esophageal pressure: a bench experiment and clinical study," BMC anesthesiology, vol. 18, pp. 1-9, 2018.
- B. C. Fortune, "Electrode–skin impedance compensation for improved bioelectrical signal acquisition," 2020.
- C. J. Cameron, C. G. Pretty, P. Bagshaw, J. Aramowicz, and M. P. Hayes, "Evaluating heart-rate variability metrics as a measure of stress during unsedated medical procedures," in International Design Engineering Technical Conferences and Computers and Information in Engineering Conference, 2023, vol. 87356: American Society of Mechanical Engineers, p. V007T07A020.
- B. C. Fortune, C. G. Pretty, L. T. Chatfield, L. R. McKenzie, and M. P. Hayes, "Low-cost active electromyography," HardwareX, vol. 6, p. e00085, 2019.
- J. D. C. Campbell, "Development of non-invasive, optical methods for central cardiovascular and blood chemistry monitoring," 2022.
- J. D. Campbell, L. Holder-Pearson, C. G. Pretty, P. Bones, and J. G. Chase, "Pulse wave velocity measurement in the carotid artery using an LED-LED array pulse oximeter," IFAC-PapersOnLine, vol. 53, no. 2, pp. 16031-16036, 2020.
- E. F. S. Guy et al., "Respiratory monitoring dataset, with rapid expiratory occlusions, over increasing positive airway pressure ventilation," Data in Brief, p. 109874, 2023/12/01/ 2023, doi: https://doi.org/10.1016/j.dib.2023.109874.
- E. F. S. Guy et al., "Respiratory dataset from PEEP study with expiratory occlusion," PhysioNet, vol. 1.0.0, 10 Nov 2023 2023, doi: https://doi.org/10.13026/d767-e709.
- E. F. Guy, J. L. Knopp, T. Lerios, and J. G. Chase, "Airflow and dynamic circumference of abdomen and thorax for adults at varied continuous positive airway pressure ventilation settings and breath rates," Scientific Data, vol. 10, no. 1, p. 481, 2023.
- E. F. Guy, J. L. Knopp, O. Gilbertson, S. Blue, L. Holder-Pearson, and J. G. Chase, "CPAP pressure and flow data at 2 positive pressure levels and multiple controlled breathing rates from a trial of 30 adults," BMC Research Notes, vol. 15, no. 1, pp. 1-3, 2022.
- E. F. S. Guy, J. Knopp, T. Lerios, and J. G. Chase, "Pressure, flow, and dynamic thoraco-abdominal circumferences data for adults breathing under CPAP therapy," PhysioNet, 2023, doi: https://doi.org/10.13026/25q9-y416.
- E. Guy, J. Knopp, and G. Chase, "CPAP Pressure and Flow Data from a Local Trial of 30 Adults at the University of Canterbury," PhysioNet, 2022, doi: https://doi.org/10.13026/xfae-vv63.
- E. Guy, J. Clifton, J. Knopp, L. Holder-Pearson, and G. Chase, "Respiratory pressure and split flow data collection device with rapid expiratory shuttering," Mendeley Data, 2023, doi: 10.17632/7mshy2kcf3.3.
Access
Access Policy:
Anyone can access the files, as long as they conform to the terms of the specified license.
License (for files):
Creative Commons Attribution 4.0 International Public License
Discovery
DOI (version 1.0.0):
https://doi.org/10.13026/e4dt-f689
DOI (latest version):
https://doi.org/10.13026/cpeg-7b46
Corresponding Author
Files
Total uncompressed size: 5.3 GB.
Access the files
- Download the ZIP file (3.1 GB)
-
Download the files using your terminal:
wget -r -N -c -np https://physionet.org/files/respiratory-heartrate-dataset/1.0.0/
| Name | Size | Modified |
|---|---|---|
| Code | ||
| EIT_rawData | ||
| HRM_rawData | ||
| PQ_rawData | ||
| Processed_Dataset | ||
| Figure1.png (download) | 303.1 KB | 2024-01-10 |
| Figure2.png (download) | 248.8 KB | 2024-01-10 |
| Figure3.png (download) | 221.7 KB | 2024-01-10 |
| LICENSE.txt (download) | 14.5 KB | 2024-03-19 |
| README.txt (download) | 6.6 KB | 2024-02-23 |
| SHA256SUMS.txt (download) | 29.5 KB | 2024-03-20 |
| subject-info.csv (download) | 28.8 KB | 2023-12-22 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}