Database Open Access
Respiratory dataset from PEEP study with expiratory occlusion
Ella Frances Sophia Guy , Jaimey Anne Clifton , Trudy Caljé-van der Klei , Rongqing Chen , Jennifer Knopp , Knut Moeller , James Geoffrey Chase
Published: Nov. 10, 2023. Version: 1.0.0
When using this resource, please cite:
(show more options)
Guy, E. F. S., Clifton, J. A., Caljé-van der Klei, T., Chen, R., Knopp, J., Moeller, K., & Chase, J. G. (2023). Respiratory dataset from PEEP study with expiratory occlusion (version 1.0.0). PhysioNet. https://doi.org/10.13026/d767-e709.
Please include the standard citation for PhysioNet:
(show more options)
Goldberger, A., Amaral, L., Glass, L., Hausdorff, J., Ivanov, P. C., Mark, R., ... & Stanley, H. E. (2000). PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation [Online]. 101 (23), pp. e215–e220.
Abstract
A trial was conducted to collect gauge pressure and flow from a venturi-based flow-meter, dynamic abdominal and thoracic circumference from rotary-encoder based tape measures, and aeration data from electrical impedance tomography (EIT). Data was collected from 80 adults, breathing with continuous positive airway pressure (CPAP) ventilation, under ethical consent from the University of Canterbury Human Research Ethics Committee (HREC 2023/04/LR-PS). In each subject’s recording the positive end expiratory pressure (PEEP) was increased from 4 to 12 cmH2O in 0.5 cmH2O increments, with data recorded for 30 seconds at each level. Time was built in for researchers to change PEEP settings, in which data continued to be collected. The recording also begins and ends with a 60 second period of breathing without CPAP. During the trial subjects breathed through a full-face mask and filter collected to the data collection device and, when PEEP was applied, CPAP circuitry. A camera-shutter based device was used to rapidly occlude the expiratory pathway to enable identification of passive lung mechanics. Subjects were instructed to breathe normally throughout the trial. Both raw and processed data is included in this publication to maximise its utility. Subject demographic data was self-reported using a questionnaire completed prior to each trial and is collated in a spreadsheet as part of this dataset. The demographic data collected was as follows: sex; height; weight; age; any history of asthma; smoking, or vaping; and resting chest width and depth. Ultimately, this dataset was collected to enable the development and validation of model-based respiratory function assessment methods. These methods aim to increase the capacity of automated testing, removing clinical burden of respiratory monitoring and improving patient-specific care.
Background
The increasing burden of respiratory disease to healthcare systems is a key driving factor in respiratory model development, to automate and better inform patient-specific care [1, 2]. The collection of respiratory datasets is critical to develop and validate these models. Outlined, is an 80 subject respiratory dataset of asthmatics, smokers, vapers, or otherwise healthy people (split evenly by sex).
Mechanically, respiration is driven by muscular recruitment which increases thoracic volume, driving flow into the lungs, and in active expiration forcing an exhalatory flow by decreasing lung volume [3, 4]. Elastic tissue mechanics impede expansion and drive passive expiration [5-7]. Airway resistances limit flow in both inhalation and exhalation [4, 5, 8]. Mechanical dysfunction can therefore be considered as either obstructive or restrictive, and to increase airway resistance or stiffen lung tissue, respectively [9-12].
Non-invasive mechanical ventilation (NIMV) is used to assist a person’s spontaneous breathing [6, 13, 14]. Continuous positive airway pressure therapy (CPAP) is the most common form of NIMV and maintains a set positive end expiratory pressure (PEEP) [15-17]. CPAP is most frequently used during sleep to reduce obstructive abnormalities exacerbated by muscular decruitment in sleep [15].
Pulmonary mechanics models can be used to detect obstructive or restrictive abnormalities, to control mechanical ventilation, and to inform patient-specific care [5, 18-23]. However, in basic physiological models with clinical applicability, eliminating trade off in identified mechanics can be difficult [24-26]. Specifically, in quiet passive breathing and CPAP, where airway pressure changes are minimal [24, 25, 27].
The ‘interrupter technique’ has been used to identify passive mechanics (elastance and resistance) by occluding expiration for 100ms [28-30]. However, the implementation of this technique results in additional patient effort to compensate and react to this expiratory flow limitation, which has previously affected model outcomes [28-30]. Therefore, a shutter-based rapid expiratory occlusion (REO) device was manufactured to occlude the airway for a shorter instance [31]. The theory being, that the initial occlusion response can be used to predict the response to a longer occlusion. Thus, REO instances can be used to model the elastance and resistance without generating an additional patient-effort response to the occlusion. Normal passive breathing is predominantly generated by diaphragmatic motion [3, 4]. However, disease and other dysfunction can cause disordered breathing patterns and shifts in ratios of thoracic and abdominal motion [32].
Muscular recruitment and elastic mechanics vary between these breathing modes and impact the application and development of pulmonary mechanics models. Dynamic circumference digital tape measures have been developed and implemented to assess changes in breathing modality in order to account for these mechanics [33]. Electrical impedance tomography (EIT) models enable non-invasive assessment of aeration [34]. EIT can assess regional aeration over the thoracic cross-section [34]. Hence, EIT gives an assessment of regional abnormalities, and their response to PEEP. Additionally global changes in aeration provide a validation metric for tidal volume computed from flow measurements.
Methods
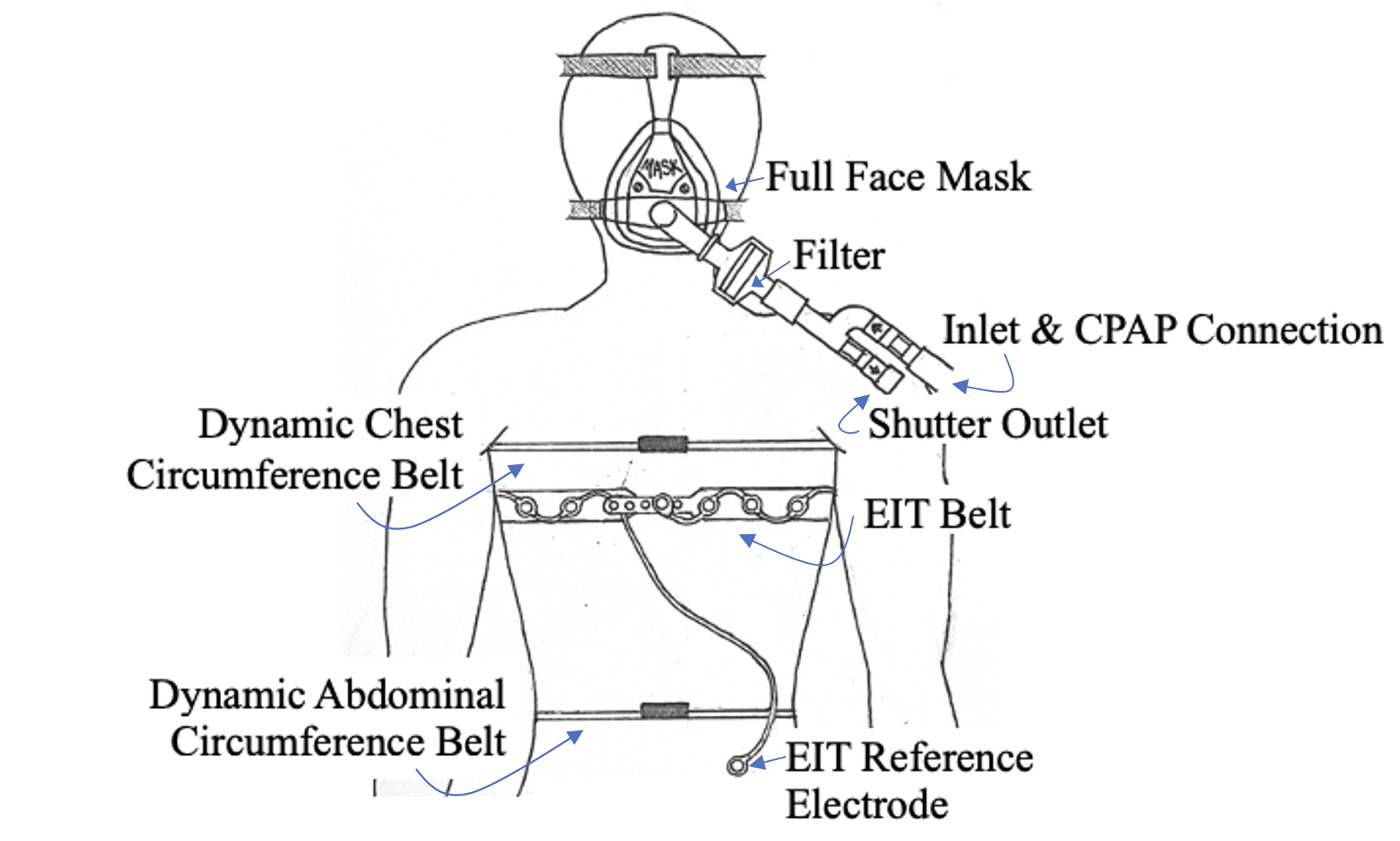
Data was primarily collected through a custom calibrated venturi-based flow and pressure sensor device [31], with attached dynamic circumference tapes around the chest and abdomen [33]. The device split inspiration and expiration pathways using one-way valves and rapidly occluded the expiratory pathway [31]. A filter and full-face mask were connected in series at the patient interface (Figure 1). The resistance of the filter was measured to average 0.5 cmH2Os/L. A CPAP machine (SleepStyle SPSCAA, Fisher and Paykel Healthcare, East Tamaki, Auckland, NZ) was connected to the inlet to provide PEEP.
Aeration data was simultaneously collected from an electrical impedance tomography (EIT) device (Dräger PulmoVista 500, Dräger, Lübeck, Germany). The EIT electrode belt was placed around the chest below the dynamic chest circumference tape (Figure 1). The subject was seated during the trial and the EIT belt was calibrated immediately prior to the trial recording commencing. EIT and circumference data was collected continuously.
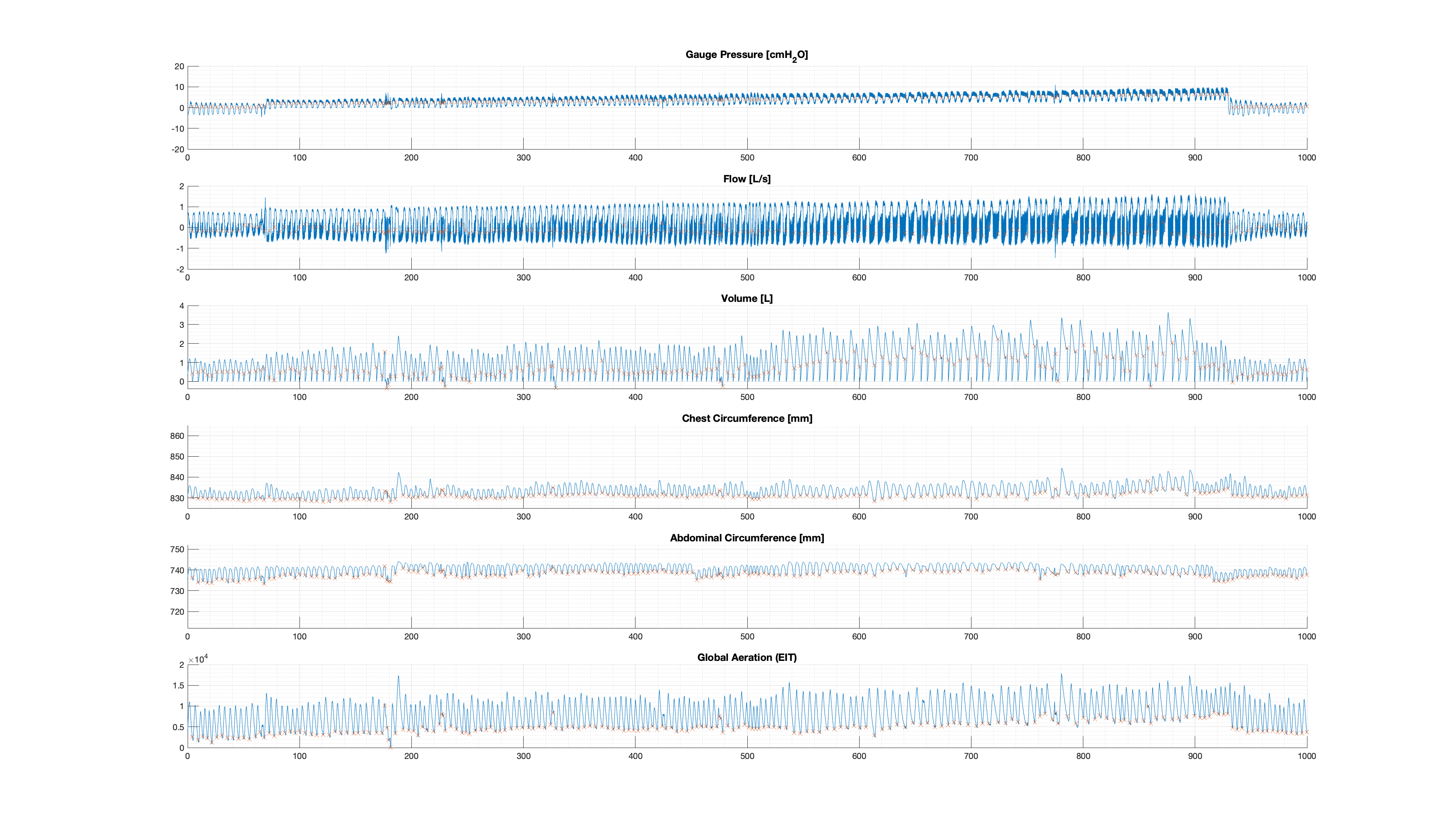
Data was collected using a MATLAB (Matlab 2021b, The Mathworks Inc, Natick, MA, USA) script, and the Dräger PulmoVista 500. In the trial data was recorded without CPAP (at ZEEP) for 1 min, then at PEEP settings of 4 through to 20 cmH2O, in increments of 0.5 cmH2O for 30 seconds, before a final 1 min recording without CPAP. 20 second windows were built into the trial schedule between PEEP settings and 30 seconds was allowed to connect and disconnect the CPAP after and before ZEEP trials. Data was collected continuously throughout the trial on both devices. Raw data from both devices was combined, aligned, and processed in MATLAB to yield processed datasets, illustrated in Figure 2 for Subject 1.
Data Description
Data from 80 subjects was collected, split evenly by sex, as well as by identification as either an asthmatic, smoker, vaper, or otherwise healthy. 'Figure-1.png' is an illustration representing the data collection systems and locations during the trial. Self-reported demographic information for the 80 subjects was collected, as well as measured initial chest width and depth. Sex [M/F], height[cm], weight [kg], age [years], and data on history of asthma, smoking, and vaping was self-reported using a questionnaire. Demographic data is collated in the 'subject-info.csv' spreadsheet by subject number.
Raw data is saved in two folders: the pressure, flow, and dynamic circumference data is saved in 'PQ_rawData'; and the EIT data is saved in 'EIT_rawData'. The 'PQ_rawData' folder contains both raw data (e.g. 'Subject1_raw.csv') and data processed into relevant units. Files are saved by subject number ('01' through to '80'). Files contain the following data sampled at 100Hz: gauge pressure; inspiratory differential pressure; expiratory differential pressure; chest circumference; abdominal circumference; initial chest cross-sectional depth; and initial chest cross-sectional width. Code to collect this data in MATLAB ('DataCollection_30MAR23.m’), and to convert files to spreadsheets ('DataConversion_07AUG23.m'), is included in the 'Code' folder. The 'EIT_rawData' contains the EIT device data, saved by subject number (e.g. 'S01_01_001_01.bin' through to 'S80_01_001_01.bin'). These files contain data as a matrix of pixel values representing regional aeration for a cross-sectional image (32x32 frame) over time (with 50Hz sampling).
Processed data is saved in the 'ProcessedDataset' folder by subject number (e.g. 'ProcessedData_Subject01.csv'). Procced data files contain: time [s]; pressure [cmH2O]; flow [L/s]; tidal volume [L]; chest circumference[mm]; abdominal circumference [mm]; inspiratory indices; aeration data time array [s]; global aeration; and aeration data inspiratory indices. Processing code ('DataProcessing_02AUG23.m') and a function to read EIT device files ('read_binData.m') is included in the ‘Code’ folder. An example figure of the processed dataset is also included ('figure-2.png') alongside figure generation code ('FigureGenerationCode_06AUG23.m').
Usage Notes
This dataset was collected to be used for the development and validation of pulmonary mechanics models. REO instances will also provide data to assess the efficacy of this method of identification of passive mechanics (elastance and resistance). The inclusion of asthmatics, smokers, and vapers in this trial aims to further investigate initial trends in work of breathing (WOB) seen in a couple of asthmatics included in previous trials [27, 35, 36]. This larger and more comprehensive dataset will enable the initial assessment of these potential trends in comparison with EIT aeration data.
The trial was conducted under University of Canterbury Human Research Ethics Committee (HREC) ethical consent (HREC 2023/04/LR-PS). The trial was conducted using hardware and code that has been made open access, with design files and instructions available [31, 33], and so can be reproduced, augmented, and modified easily for future research applications. MATLAB data collection code, processing and functions, and example figure generation code has also been included in this dataset.
Ethics
Ethical consent for the trial was granted by the Human Research Ethics Committee at the University of Canterbury (Ref: HREC 2023/04/LR-PS), with amendments accepted on 24 March 2023.
Acknowledgements
This work was funded by a University of Canterbury Doctoral Scholarship and the EU H2020 R&I programme (MSCA-RISE-2019 call) under grant agreement #872488 — DCPM.
Conflicts of Interest
The authors have no conflcits of interest to declare.
References
- P. Burney, D. Jarvis, and R. Perez-Padilla, "The global burden of chronic respiratory disease in adults," The International Journal of Tuberculosis and Lung Disease, vol. 19, no. 1, pp. 10-20, 2015.
- L. Dwyer-Lindgren et al., "Trends and patterns of differences in chronic respiratory disease mortality among US counties, 1980-2014," Jama, vol. 318, no. 12, pp. 1136-1149, 2017.
- J. B. West and A. M. Luks, West's Respiratory Physiology. Lippincott Williams & Wilkins, 2020.
- G. J. Tortora and B. H. Derrickson, Principles of anatomy and physiology. John Wiley & Sons, 2018.
- J. H. Bates, Lung mechanics: an inverse modeling approach. Cambridge University Press, 2009.
- A. B. Lumb and C. R. Thomas, Nunn's applied respiratory physiology eBook. Elsevier Health Sciences, 2020.
- J. B. West, Pulmonary pathophysiology: the essentials. Lippincott Williams & Wilkins, 2008.
- N. S. Damanhuri, Y. S. Chiew, P. Docherty, P. Geoghegan, and G. Chase, "Respiratory airway resistance monitoring in mechanically ventilated patients," in 2012 IEEE-EMBS Conference on Biomedical Engineering and Sciences, 2012: IEEE, pp. 311-315.
- T. Des Jardins and G. G. Burton, Clinical Manifestations & Assessment of Respiratory Disease-E-Book. Elsevier Health Sciences, 2023.
- J. Butler, C. G. Caro, R. Alcala, and A. B. DuBois, "Physiological factors affecting airway resistance in normal subjects and in patients with obstructive respiratory disease," The Journal of clinical investigation, vol. 39, no. 4, pp. 584-591, 1960.
- L. C. Melo, M. A. M. d. Silva, and A. C. d. N. Calles, "Obesity and lung function: a systematic review," Einstein (Sao Paulo), vol. 12, pp. 120-125, 2014.
- V. S. Taskar and D. B. Coultas, "Is idiopathic pulmonary fibrosis an environmental disease?," Proceedings of the American Thoracic Society, vol. 3, no. 4, pp. 293-298, 2006.
- M. B. Amato, C. S. Barbas, J. Bonassa, P. H. Saldiva, W. A. Zin, and C. R. de Carvalho, "Volume-assured pressure support ventilation (VAPSV). A new approach for reducing muscle workload during acute respiratory failure," (in eng), Chest, vol. 102, no. 4, pp. 1225-34, Oct 1992, doi: 10.1378/chest.102.4.1225.
- E. L'Her et al., "Physiologic effects of noninvasive ventilation during acute lung injury," vol. 172, no. 9, pp. 1112-1118, 2005.
- N. Stasche, "Selective indication for positive airway pressure (PAP) in sleep-related breathing disorders with obstruction," GMS Current Topics in Otorhinolaryngology, Head and Neck Surgery, vol. 5, 2006.
- T. Theerakittikul, B. Ricaurte, and L. S. J. C. C. J. M. Aboussouan, "Noninvasive positive pressure ventilation for stable outpatients: CPAP and beyond," vol. 77, no. 10, pp. 705-714, 2010.
- A. M. Miro, M. R. Pinsky, and P. L. Rogers, "Effects of the components of positive airway pressure on work of breathing during bronchospasm," (in eng), Crit Care, vol. 8, no. 2, pp. R72-81, Apr 2004, doi: 10.1186/cc2461.
- J. G. Chase et al., "Next-generation, personalised, model-based critical care medicine: a state-of-the art review of in silico virtual patient models, methods, and cohorts, and how to validation them," Biomedical engineering online, vol. 17, no. 1, pp. 1-29, 2018.
- Y. S. Chiew, J. G. Chase, G. M. Shaw, A. Sundaresan, and T. Desaive, "Model-based PEEP optimisation in mechanical ventilation," Biomedical engineering online, vol. 10, pp. 1-16, 2011.
- Y. S. Chiew et al., "Time-varying respiratory system elastance: a physiological model for patients who are spontaneously breathing," PloS one, vol. 10, no. 1, p. e0114847, 2015.
- S. E. Morton et al., "Optimising mechanical ventilation through model-based methods and automation," Annual Reviews in Control, vol. 48, pp. 369-382, 2019.
- S. E. Rees et al., "Using physiological models and decision theory for selecting appropriate ventilator settings," Journal of clinical monitoring and computing, vol. 20, pp. 421-429, 2006.
- S. E. Rees, "The Intelligent Ventilator (INVENT) project: The role of mathematical models in translating physiological knowledge into clinical practice," Computer methods and programs in biomedicine, vol. 104, pp. S1-S29, 2011.
- E. F. Guy, J. G. Chase, J. L. Knopp, and G. M. Shaw, "Quantifying ventilator unloading in CPAP ventilation," Computers in Biology and Medicine, vol. 142, p. 105225, 2022.
- E. F. Guy, J. L. Knopp, and J. G. Chase, "Pilot study of model-based estimation of inspiratory driving pressure in CPAP ventilation," IFAC-PapersOnLine, vol. 54, no. 15, pp. 109-114, 2021.
- J. L. Knopp, E. Guy, K. T. Kim, G. M. Shaw, and J. G. Chase, "B-spline modelling of inspiratory drive in NAVA-ventilated patients," IFAC-PapersOnLine, vol. 54, no. 15, pp. 103-108, 2021.
- E. F. S. Guy, J. L. Knopp, T. Lerios, and J. G. Chase, "Model-based Identification of Work of Breathing in CPAP Ventilation of Healthy Adults " IFAC-PapersOnLine vol. In Review, 2023.
- P. Panagou, I. Kottakis, A. Tzouvelekis, S. Anevlavis, and D. Bouros, "Use of interrupter technique in assessment of bronchial responsiveness in normal subjects," BMC Pulmonary Medicine, vol. 4, no. 1, pp. 1-6, 2004.
- E. Y.-T. Chan, "Use of the interrupter technique in assessment of lung function," J Paediatr Respirol Crit Care, vol. 3, no. 4, pp. 6-8, 2007.
- S. L. Howe et al., "Measuring lung mechanics of expiratory tidal breathing with non-invasive breath occlusion," BioMedical Engineering OnLine, vol. 19, no. 1, p. 32, 2020.
- E. F. S. Guy, J. A. Clifton, J. L. Knopp, L. R. Holder-Pearson, and J. G. Chase1, "Respiratory pressure and split flow data collection device with rapid occlusion attachment," HardwareX, vol. In Review, 2023.
- N. Barker and M. L. Everard, "Getting to grips with ‘dysfunctional breathing’," Paediatric respiratory reviews, vol. 16, no. 1, pp. 53-61, 2015.
- E. F. Guy, J. G. Chase, and L. R. Holder-Pearson, "Respiratory bi-directional pressure and flow data collection device with thoracic and abdominal circumferential monitoring," HardwareX, vol. 12, p. e00354, 2022.
- M. Kidwai, "PULMOVISTA 500 BY DRAGER: A SNAPSHOT OF CLINICAL USABILITY IN THE ICU SETTING," Canadian Journal of Respiratory Therapy, vol. 57, 2021.
- E. F. Guy, J. L. Knopp, T. Lerios, and J. G. Chase, "Airflow and dynamic circumference of abdomen and thorax for adults at varied continuous positive airway pressure ventilation settings and breath rates," Scientific Data, vol. 10, no. 1, p. 481, 2023.
- E. F. S. Guy, J. Knopp, T. Lerios, and J. G. Chase, "Pressure, flow, and dynamic thoraco-abdominal circumferences data for adults breathing under CPAP therapy," PhysioNet, 2023, doi: https://doi.org/10.13026/25q9-y416.
Access
Access Policy:
Anyone can access the files, as long as they conform to the terms of the specified license.
License (for files):
Creative Commons Attribution 4.0 International Public License
Discovery
DOI (version 1.0.0):
https://doi.org/10.13026/d767-e709
DOI (latest version):
https://doi.org/10.13026/psrj-rw40
Corresponding Author
Files
Total uncompressed size: 18.3 GB.
Access the files
- Download the ZIP file (14.2 GB)
-
Download the files using your terminal:
wget -r -N -c -np https://physionet.org/files/respiratory-dataset/1.0.0/
| Name | Size | Modified |
|---|---|---|
| Code | ||
| EIT_rawData | ||
| PQ_rawData | ||
| Processed_Dataset | ||
| LICENSE.txt (download) | 14.5 KB | 2023-11-10 |
| README.txt (download) | 4.1 KB | 2023-11-02 |
| SHA256SUMS.txt (download) | 31.2 KB | 2023-11-10 |
| figure-1.png (download) | 469.3 KB | 2023-08-30 |
| figure-2.png (download) | 426.8 KB | 2023-08-29 |
| subject-info.csv (download) | 78.8 KB | 2023-05-30 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}