Database Open Access
Induced Cesarean EHG DataSet (ICEHG DS): An open dataset with electrohysterogram records of pregnancies ending in induced and cesarean section delivery
Published: Oct. 8, 2023. Version: 1.0.1
When using this resource, please cite:
(show more options)
Jager, F. (2023). Induced Cesarean EHG DataSet (ICEHG DS): An open dataset with electrohysterogram records of pregnancies ending in induced and cesarean section delivery (version 1.0.1). PhysioNet. https://doi.org/10.13026/zw34-n382.
Please include the standard citation for PhysioNet:
(show more options)
Goldberger, A., Amaral, L., Glass, L., Hausdorff, J., Ivanov, P. C., Mark, R., ... & Stanley, H. E. (2000). PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation [Online]. 101 (23), pp. e215–e220.
Abstract
The surface electrohysterogram (EHG) has emerged as a promising diagnostic tool for non-invasive automated preterm birth prediction. The existing automated preterm birth prediction methods rely on the use of uterine EHG records coming from spontaneous preterm and term deliveries, and are indifferent to term induced and cesarean deliveries. In order to enhance current publicly available pool of term EHG records, we developed a new EHG dataset containing 126 30-minute EHG records, recorded either early (23rd week), or later during pregnancy (31st week), of those pregnancies that were expected to end in spontaneous term delivery, but ended in induced or cesarean section delivery. The records were collected at the University Medical Center Ljubljana, Ljubljana, Slovenia. The dataset includes 38 and 43, early and later, induced; 11 and 8, early and later, cesarean; and 13 and 13, early and later, induced-cesarean records. This database enables better understanding of the underlying physiological mechanisms involved during pregnancies ending in induced and cesarean deliveries, and provides more robust and realistic assessment of the performance of automated preterm birth prediction.
Background
Current existing methods using uterine EHG records for predicting preterm birth solely base on classifiation between EHG records of which pregnancies ended in preterm spontaneous or term spontaneous delivery mode, and do not take into account other delivery modes like induced or cesarean section delivery. A robust and realistic approach for accurate prediction of preterm birth that base on the analysis of EHG records should take into account also the characteristics of EHG records of term induced and term cesarean section deliveries. Moreover, in the last 10 years the number of induced and cesarean deliveries has increased even if there is no apparent medical reason [1,2]. The latest related studies, using EHG records of induced or cesarean section delivery modes, focuses on characterization and differentiation of antepartum, labor, and post-partum records [3], differentiation between term spontaneous labor and induced late-term labor [4], prediction of labor induction success in the first hours after induction of labor [5], and prediction of cesarean section and spontaneous vaginal delivery modes [6]. However, these delivery-mode prediction methods relied on antepartum or labor EHG records, after the 37th week of gestation, and did not take into account early (23rd week) or later (31st week) recorded EHG records, nor preterm birth prediction.
For these reasons we developed a new EHG dataset with term induced, cesarean, and induced-cesarean EHG records, i.e., Induced Cesarean EHG DataSet (ICEHG DS) [7]. We used the same acquisition protocol and the same recording device as were used for obtaining uterine EHG records of our previously developed TPEHG DB [8] and TPEHGT DS [9]. The ICEHG DS contains 126 EHG records (91 pregnancies), recorded around the 23rd and/or 31st week of pregnancy, of induced, cesarean, and induced and cesarean deliveries. Publicly available ICEHG DS allows researchers further studies in order to answer the following important questions: 1) Can the induced and cesarean section delivery modes be predicted early, already in the 23rd, or in 31st week of pregnancy? and, 2) Can the characteristics of the EHG records of induced and cesarean section delivery modes influence the understanding of the underlying mechanisms involved during pregnancy, and more important, the understanding of the mechanisms responsible for preterm birth? Moreover, the ICEHG DS, used alongside TPEHG DB and TPEHGT DS, will provide more robust and realistic assessment of the performance of automated preterm birth prediction.
Methods
Data collecting
In the period from 1997 and 2006, a large number of uterine EHG records (a total of 1,211) were collected at the Clinical Department of Perinatology, University Medical Center Ljubljana, Ljubljana, Slovenia. Records were collected from the general population during routine checkups, and from the patients admitted to the hospital with the diagnosis of impending preterm labor. The records were collected either early, around the 23rd week of gestation (early records), and/or later in the pregnancy, around the 31st week of gestation (later records). From this entire pool of uterine EHG records, in 2011 and in 2018, we developed the TPEHG DB [8] and TPEHGT DS [9], respectively, and made them publicly available in the PhysioNet repository. At that times, we were interested only in those EHG records with spontaneous preterm and spontaneous term delivery, and not in those ending in induced or cesarean section delivery.
The EHG records selected for the Induced Cesarean EHG DataSet (ICEHG DS) are also coming from the pool of EHG records collected between 1997 and 2006. Obtaining of the uterine EHG records was approved by the National Medical Ethics Committee of the Republic of Slovenia (No. 32/01/97). All women gave their written signed consent. The selected records for the ICEHG DS are those collected for the pregnancies which were expected to have a normal progression toward the spontaneous start of labor and vaginal term delivery, but ultimately ended either in term vaginal delivery that failed to start spontaneously and labor had to be induced (induced records), in term delivery by emergency cesarean section without prior induction of labor (cesarean records), or in term delivery by emergency cesarean section after a failed induction (induced-cesarean records).
Recording protocol
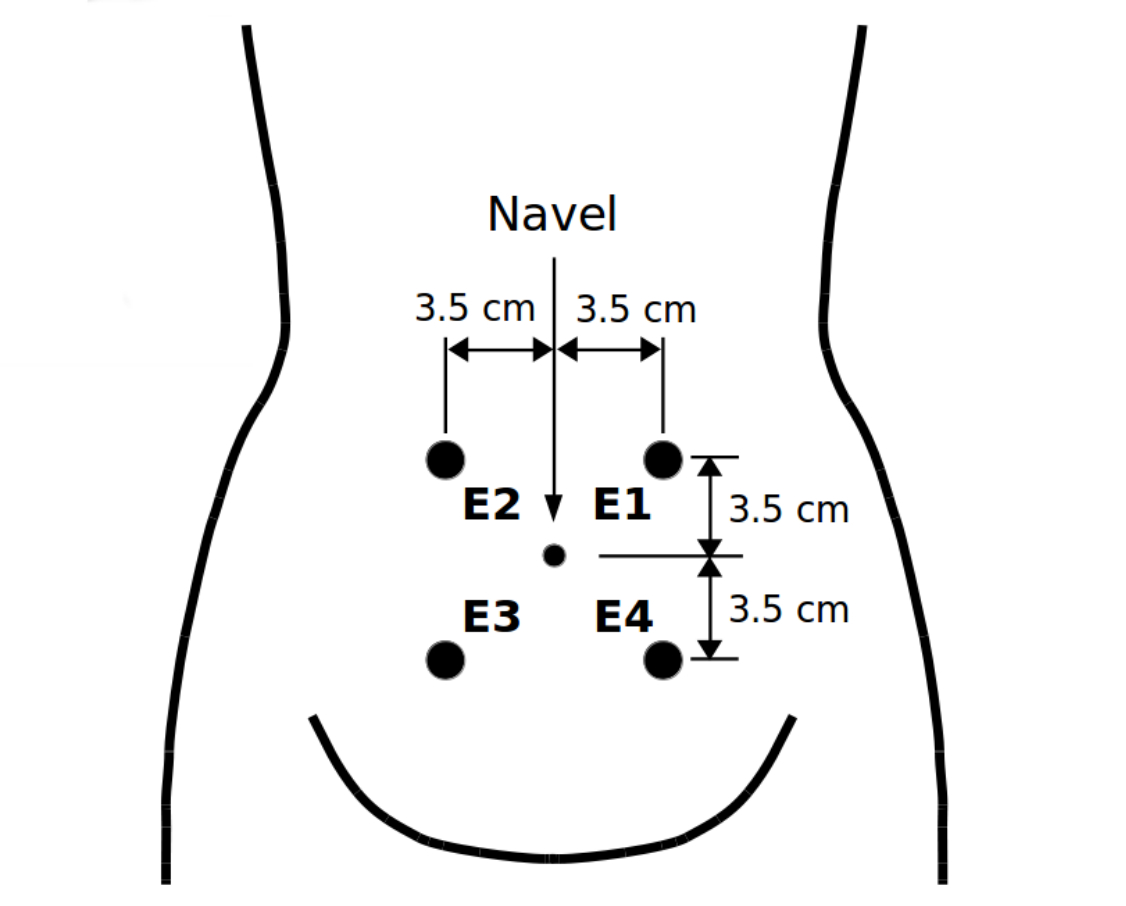
The recording protocol and the recording equipment were those which were also used during collecting the records of the TPEHG DB and TPEHGT DS. The records were collected from the abdominal surface using four Ag2Cl electrodes. The electrodes were placed symmetrically above and under the navel, at the distance of 7 cm (see Figure 1).
The acquired EHG records are of length of approximately 30 minutes and consist of three bipolar EHG signals. The first acquired bipolar EHG signal was measured between the upper two electrodes, S1 = E2 - E1, the second bipolar EHG signal between the left two electrodes, S2 = E2 - E3, and the third bipolar EHG signal between the lower two electrodes, S3 = E4 - E3. Prior to sampling, the signals were filtered using an analog anti-aliasing low pass three-pole Butterworth filter with the cutt-off frequency of 5.0 Hz. The sampling frequency, Fs, was 20 Hz. The resolution of the signal acquisition equipment was 16 bits with the amplitude range of ±2.5 mV (A/D value of 13107 units corresponds to 1.0 mV).
Data processing
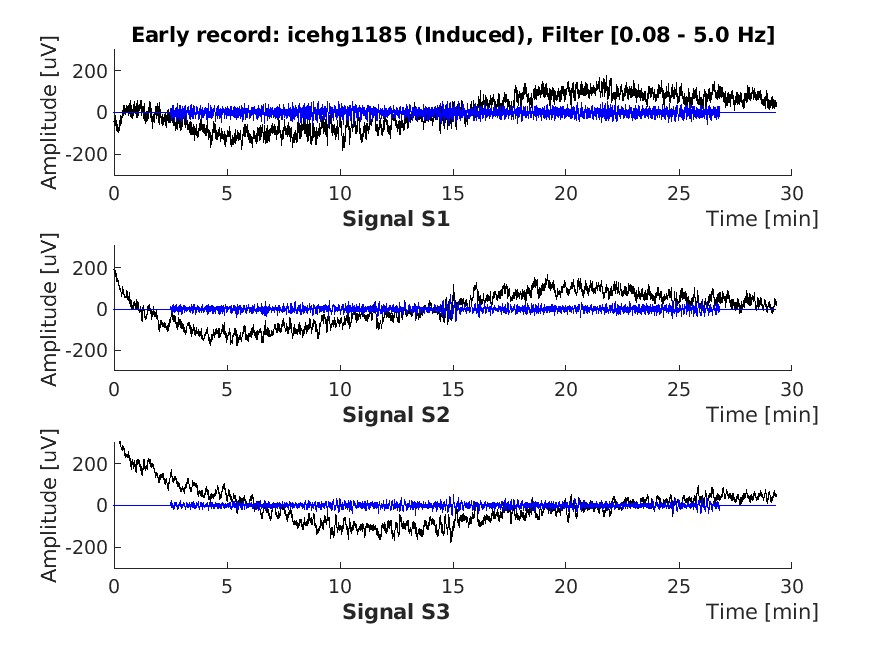
In order to provide additional version of the EHG signals of the uterine EHG records obtained during recording without extremely slow signal drifts (the analog anti-aliasing filter passed frequencies from 0.0-5.0 Hz), the original EHG signals were filtered using a four-pole digital band-pass Butterworth filter with the cut-off frequencies at 0.08 Hz and 5.0 Hz, applied bidirectionally to eliminate the non-linear phase shift. An example of the EHG signals prior to and after this filtering for a selected record of the ICEHG DS is shown in Figure 2. (Signal samples of the first and last 150 seconds of the filtered signals are set to zero.)
Data Description
All together, the ICEHG DS contains 126 three-signal 30-minute surface EHG records coming from 91 pregnancies that were recorded early, around the 23rd week (62 records), and later, around the 31st week (64 records), of pregnancy. Precisely, the dataset includes 38 and 43, early and later, induced EHG records of 59 pregnancies (see Table 1); 11 and 8, early and later, cesarean EHG records of 13 pregnancies (see Table 2); and 13 and 13, early and later, induced-cesarean EHG records of 19 pregnancies (see Table 3). The mean times of gestation in weeks were 39.8 ± 1.4 for induced, 39.7 ± 1.1 for cesarean, and 39.4 ± 0.9 for induced-cesarean records.
The records are in the PhysioNet's WFDB format and are stored in the two-level directory structure (root directory containing single-level sub-directories). The records are stored in the following sub-directories with regard to the period of recording and according to the delivery mode:
early_induced(38 induced EHG records recorded around the 23rd week);early_cesarean(11 cesarean EHG records recorded around the 23rd week);early_induced-cesarean(13 induced-cesarean EHG records recorded around the 23rd week);later_induced(43 induced EHG records recorded around the 31st week);later_cesarean(8 cesarean EHG records recorded around the 31st week);later_induced-cesarean(13 induced-cesarean EHG records recorded around the 31st week).
Names of the records are the following: icehgXXX[X], where XXX[X] represents record ID.
The list of all EHG records is contained in the ASCII file named RECORDS. The lists of records for the groups of EHG records per delivery mode (induced, cesarean, or induced-cesarean) are contained in the accompanied ASCII files named:
RECORDS_induced(names of all induced EHG records);RECORDS_cesarean(names of all cesarean EHG records);RECORDS_induced-cesarean(names of all induced-cesarean EHG records).
Each raw in these three files corresponds to a pregnancy and contains the name (and sub-directory name) of early and/or name (and sub-directory name) of later EHG record of the pregnancy, given the delivery mode; while if considering columns in these three files, the first column contains the names of all early EHG records, and the second column the names of all later EHG records, given the delivery mode. A zero indicates that no early, or later, EHG record for that pregnancy exists.
Each EHG record is composed from the following three files:
1. A figure (icehgXXX[X]_fltrd.jpg) showing the three original EHG signals and their filtered versions (an example is shown in Figure 2).
2. A binary signal data file (icehgXXX[X].dat) containing the three original EHG signals (S1, S2, and S3) and their filtered versions.
The signal data in these data files are in the WFDB format and are in the following order:
- Original, unfiltered, signal S1;
- filtered signal S1 using a four-pole band-pass Butterworth filter from 0.08 Hz to 5.0
Hz applied bidirectionally; - original, unfiltered, signal S2;
- filtered signal S2 using a four-pole band-pass Butterworth filter from 0.08 Hz to 5.0
Hz applied bidirectionally; - original, unfiltered, signal S3.
- filtered signal S3 using a four-pole band-pass Butterworth filter from 0.08 Hz to 5.0
Hz applied bidirectionally.
3. A header ASCII file (icehgXXX[X].hea) containing the general data of the record and accompanied clinical information of the participant.
The top most part of the header files is the general data of the record according to the WFDB format including: record name, sampling frequency, length of the record in samples, list of signals with their specifications according to the WFDB format, calibration constants, and signal labels. The rest of the header files is the comments section containing the accompanied clinical information of the participant. This comments section contains the following information:
RecIDrecord ID;RecTypetype of delivery (Induced, Cesarean, or Induced-cesarean);Gestationgestational age in weeks;Rectimerecording time in weeks;Ageage of the participant in years;Weightweight at the recording time in kg;Placental_positionplacental position (front/end);Heightheight of the participant in cm;Newborn_weightnewborn weight in g;Pair_RecIDID of the pair record.
Tables 1, 2, and 3 contain the general data and accompanied clinical information (the contents of the comments section of the .hea files) of the participants ending in induced (Table 1), cesarean (Table 2), and induced-cesarean (Table 3) delivery.
The records of the ICEHG DS are also available in MATLAB format in the sub-directory named icehgdsmat containing .mat signal and .hea header files.
Usage Notes
The ICEHG DS is intended to study physiological mechanisms involved during pregnancy that lead to induction, cesarean section, or both. Characterization and separation of the EHG records of the ICEHG DS can answer the question whether the induced and cesarean section delivery modes can be predicted early, already in the 23rd, or later, in the 31st week of pregnancy.
Furthermore, the ICEHG DS is intended to provide more realistic pool of EHG records ending in term delivery. Since the same acquisition protocol and the same recording device were used in the TPEHG DB [8], TPEHGT DS [9], and in ICEHG DS, the EHG records of the ICEHG DS can be used alongside term spontaneous, early and later, EHG records of the TPEHG DB and TPEHGT DS to better understand the underlying physiologic mechanisms leading to different kinds of term delivery modes. Furthermore, adding the preterm spontaneous EHG records of the TPEHG DB and TPEHGT DS can answer the question how the characteristics of EHG records of the induced and cesarean section delivery modes influence the understanding of the underlying mechanisms responsible for preterm birth. Such a composed pool of EHG records from all three database/datasets can provide a robust and more realistic evaluation of non-invasive automatic or semi-automatic methods for predicting preterm birth. To address some of these questions, the records of the ICEHG DS, alongside the EHG records of the TPEHG DB and TPEHGT DS, have already successfully been used in one of our studies [10]. Characterization and separation of all later recorded preterm and term spontaneous, induced, cesarean, and induced and cesarean, groups of EHG records of these three database/datasets, showed that the peak amplitude of the normalized power spectra of EHG signals in the frequency band 0.125–0.575 Hz (which approximately matches the Fast Wave Low band), efficiently separate between the later preterm group and all other later term delivery groups, and efficiently separate between the later preterm group and any of other later term delivery groups.
The potential for the ICEHG DS reuse are the following:
- Study of the physiological mechanisms involved during pregnancy that lead to induction,
cesarean section, or both; - early prediction (in the 23rd or 31st week of pregnancy) of the induced and
cesarean section delivery modes; - assessing the classification performance (alongside TPEHG DB and TPEHGT DS) to classify
between all early and/or later recorded preterm and term spontaneous, induced, cesarean,
and induced and cesarean groups of EHG records.
In the EHG records of the ICEHG DS, three bipolar original EHG signals are stored. The first, S1, was measured between the upper two electrodes (see Figure 1), the second, S2, between the left two electrodes, and the third, S3, between the lower two electrodes. Signal S1 and signal S3 estimate uterine electrical activity in the horizontal direction, while signal S2 in the vertical direction. In order to better characterize the electrical activity in the vertical direction, the users of the ICEHG DS (and of TPEHG DB and TPEHGT DS) may synthetically derive the fourth bipolar signal, S4, to estimate the uterine electrical activity in the vertical direction between the right two electrodes E4 and E1, S4 = E4 - E1. Since S1 = E2 - E1, S2 = E2 - E3, and S3 = E4 - E3, and using E4 = S3 + E3 and E1 = E2 - S1, it follows that:
Similarly, bipolar signals estimating the uterine electrical activity in both diagonal directions, between the electrodes E2 and E4, and between the electrodes E1 and E3, can be derived. The discrepancies between synthetically derived signal, S4, and the signal as it would be actually measured between the right two electrodes E4 and E1, are negligible. The estimated discrepancy between the calculated, S4, and actually measured signal, i.e., the standard deviation between the samples of these two signals (calculated throughout the 30-minute signals), is less than the difference between two adjacent integer values (0.076 µV) of the signal amplitudes (1 mV / 13107 = 0.076 µV, where 13107 is the calibration constant relating to 1 mV), and close to the quantization error (0.038 µV) of A/D converter.
Limitations are the following:
- The unipolar EHG signals, as measured at the electrodes E1, E2, E3, and E4, are not stored in the EHG records; nor it is possible to synthetically derive them form the bipolar signals S1, S2, and S3;
- it is good idea to set the values of signal samples of the first and last 150 seconds of the filtered version of the signals to zero (or to reject them) due to the transient effects of Butterworth filter which was used bidirectionally for filtering the signals.
Ethics
Obtaining of the uterine EHG records was approved by the National Medical Ethics Committee of the Republic of Slovenia (No. 32/01/97). All women gave their written signed consent.
Acknowledgements
The design and development of the ICEHG DS was funded by the Slovenian Research Agency (ARRS) [11] under the research project Metabolic and inborn factors of reproductive health, birth III. The author would like to acknowledge the University Medical Center Ljubljana, Clinical Department of Perinatology, for their collaboration.
Conflicts of Interest
This research was funded by the Slovenian Research Agency (ARRS). The author declare no conflict of interest. The funder had no role in the design of the study; in the collection of the data; in the writing of the manuscript, or in the decision to publish the results.
References
- Antoine, C. & Young, B. K. (2020). Cesarean section one hundred years 1920–2020: The good, the bad and the ugly. Journal of Perinatal Medicine, 49(1), 5–16, https://doi.org/10.1515/jpm-2020-0305
- Dahlen, H. G., Thornton, C., Downe, S., de Jonge, A., Seijmonsbergen-Schermers, A., Tracy, S., Tracy, M., Bisits, A. & Peters, L. (2021). Intrapartum interventions and outcomes for women and children following induction of labour at term in uncomplicated pregnancies: A 16-year population-based Linked Data Study. BMJ Open 11, e047040, https://doi.org/10.1136/bmjopen-2020-047040
- Mas-Cabo, J., Ye-Lin, Y., Garcia-Casado, J., Díaz-Martinez, A., Perales-Marin, A., Monfort-Ortiz, R., Roca-Prats, A., López-Corral, A. & Prats-Boluda, G. (2020). Robust Characterization of the Uterine Myoelectrical Activity in Different Obstetric Scenarios. Entropy 22, 743, https://doi.org/10.3390/e22070743
- Alberola-Rubio, J., Garcia-Casado, J., Prats-Boluda, G., Ye-Lin, Y., Desantes, D., Valero, J. & Perales, A. (2017). Prediction of labor onset type: Spontaneous vs induced; role of electrohysterography? Computer Methods and Programs in Biomedicine 144, 127–133, https://dx.doi.org/10.1016/j.cmpb.2017.03.018
- Benalcazar-Parra, C., Ye-Lin, Y., Garcia-Casado, J., Monfort-Ortiz, R., Alberola-Rubio, J., Perales, A. & Prats-Boluda, G. (2019). Prediction of labor induction success from the uterine electrohysterogram. Journal of Sensors 2019, ID 6916251, https://doi.org/10.1155/2019/6916251
- Fergus, P., Selvaraj, M. & Chalmers, C. (2018). Machine learning ensemble modelling to classify caesarean section and vaginal delivery types using Cardiotocography traces. Computers in Biology and Medicine 93, 7–16, https://doi.org/10.1016/j.compbiomed.2017.12.002
- Jager, F. (2023). An open dataset with electrohysterogram records of pregnancies ending in induced and cesarean section delivery. Scientific Data. 10, Article number: 669, https://doi.org/10.1038/s41597-023-02581-6
- Fele-Žorž, G., Kavšek, G., Novak-Antolič, Ž. & Jager, F. (2008). A comparison of various linear and non-linear signal processing techniques to separate uterine EMG records of term and pre-term delivery groups. Med Biol Eng Comput, 46, 911–922, https://physionet.org/content/tpehgdb/1.0.1/tpehgdb.pdf
- Jager, F., Libenšek S. & Geršak, K (2018). Characterization and automatic classification of preterm and term uterine records. PLoS ONE 13(8):e0202125. https://doi.org/10.1371/journal.pone.0202125
- Pirnar, Ž., Jager, F. & Geršak, K. (2022). Characterization and separation of preterm and term spontaneous, induced, and cesarean EHG records. Computers in Biology and Medicine, 151, 106238. https://doi.org/10.1016/j.compbiomed.2022.106238
- "Slovenian Research Agency (ARRS)" https://www.arrs.gov.si/ [Accessed 08/26/2023]
Access
Access Policy:
Anyone can access the files, as long as they conform to the terms of the specified license.
License (for files):
Open Data Commons Open Database License v1.0
Discovery
DOI (version 1.0.1):
https://doi.org/10.13026/zw34-n382
DOI (latest version):
https://doi.org/10.13026/vrvd-mf28
Topics:
neuroelectric
pregnancy
electrohysterogram
cesarean-section delivery
induced delivery
Project Website:
https://lbcsi.fri.uni-lj.si/
Corresponding Author
Files
Total uncompressed size: 115.6 MB.
Access the files
- Download the ZIP file (89.0 MB)
-
Download the files using your terminal:
wget -r -N -c -np https://physionet.org/files/icehg-ds/1.0.1/
| Name | Size | Modified |
|---|---|---|
| early_cesarean | ||
| early_induced | ||
| early_induced-cesarean | ||
| icehgdsmat | ||
| later_cesarean | ||
| later_induced | ||
| later_induced-cesarean | ||
| Figure_1.jpg (download) | 106.5 KB | 2023-07-02 |
| Figure_2.jpg (download) | 112.3 KB | 2023-07-02 |
| LICENSE.txt (download) | 25.2 KB | 2023-10-08 |
| README (download) | 907 B | 2023-07-07 |
| RECORDS (download) | 3.2 KB | 2023-07-02 |
| RECORDS_cesarean (download) | 544 B | 2023-07-02 |
| RECORDS_induced (download) | 2.5 KB | 2023-07-02 |
| RECORDS_induced-ceasarean (download) | 1.1 KB | 2023-07-02 |
| SHA256SUMS.txt (download) | 63.1 KB | 2023-10-08 |
| Table_1.txt (download) | 12.3 KB | 2023-07-02 |
| Table_2.txt (download) | 4.1 KB | 2023-07-02 |
| Table_3.txt (download) | 5.2 KB | 2023-07-02 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}